
Every year on 30th November celebrated as Neuro-spinal day, last year we had discussed about low back pain. Today we are going on to another important topic of neck pain.
Neck pain is caused by numerous factors, including muscle or ligament strains, arthritis, or a “pinched” nerve (when a nerve is irritated by something pressing on it). About 10 to 20 percent of adults have neck pain at any one time. Females are affected more than males. Most of the time, pain improves with conservative therapy.
Neck pain is often categorized as “acute” (lasting less than six weeks), “subacute” (lasting 6 to 12 weeks), or “chronic” (lasting more than 12 weeks). Most episodes of acute pain resolve spontaneously, some go on to have long-term pain.
This article discusses the causes, evaluation, and available treatments for neck pain.
NECK ANATOMY
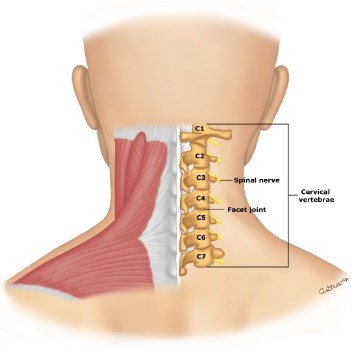
The neck, or cervical spine, is formed by seven square-shaped bones (cervical vertebrae), which are stacked one on top of another. The vertebrae are named for their position in the neck, beginning from top with C1, C2, C3, and down till C7. The skull and upper cervical vertebrae are uniquely connected to allow for movement of the skull. Together with the supporting ligaments and the overlying long neck muscles, the cervical vertebrae form a strong spinal canal that surrounds and protects the spinal cord.
Discs are found between the neck bones, which function as shock absorbers, acting like cushions between the vertebrae. Whenever there is excessive pressure on disc, the inner jelly-like material protrudes through its outer capsule which is called herniated or “slipped” disc. If a herniated disc irritates a nerve root, it can cause symptoms. Other words used to describe a disc problem include “bulging,” “protruding,” “extruded,” or “ruptured.”
Directly covering the bones and the discs is a dense layer of ligaments. These thick tissues attach directly to the bones and function to limit the movement of the cervical vertebrae against each other. Motor vehicle accidents or other trauma involving the head, neck, or upper body can cause injury to these ligaments. This “whiplash” movement of the neck can range in severity from minor bruising to complete tear and separation of ligament from the bone.
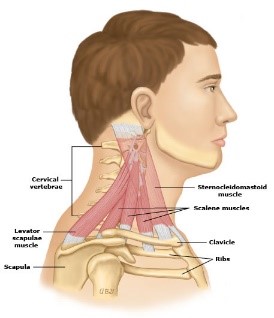
The major muscles of the neck form the next protective layer. These muscles are responsible for holding the head upright, maintaining normal posture, and supporting and moving the neck. Overuse and irritation of these muscles is referred to as neck strain or muscle tension. These problems can contribute to “muscle tension” headaches..
NECK PAIN CAUSES
There are many causes of neck pain, although it is often difficult to know with certainty what is causing pain. This is because the physical examination, and even imaging tests, are not able to easily differentiate among the various potential causes. In addition, degenerative bone and joint changes visible on imaging tests often do not correlate with the severity of pain. In other words, it is possible to have neck pain with relatively normal imaging tests, or to have no (or only mild) pain despite significant abnormalities on imaging.
Cervical strain/sprain — cervical muscle strain can occur when there is an injury to the muscles of the neck, causing spasm (sudden tightening) of the cervical and upper back muscles. Cervical strain results from physical stresses of everyday life, including poor posture, muscle tension from psychologic stress, or poor sleeping habits. Sports-related injuries can also result in cervical strain. Typically, cervical strain symptoms include pain, stiffness, and tightness in the upper back or shoulder, which may last for up to six weeks.
Cervical spondylosis — Cervical spondylosis is a condition caused by abnormal wear and tear (called degenerative changes) of the cervical spine. This leads to gradual narrowing of the disc space, a loss of the normal square-shaped bone, and bone spurs (growths at the edges of the bones). These spurs can increase pressure on the surrounding tissues and lead to pinched nerves. Some degree of wear and tear is expected with normal aging, although severe degenerative changes are not typical.
Symptoms of cervical spondylosis can include neck pain or weakness, numbness or abnormal sensations of the arms or shoulders, headaches, or limited ability to move the neck. Ear pain has also been associated with upper cervical spondylosis in some cases.
Cervical Discogenic pain — Cervical discogenic pain may be the most common cause of neck pain. It is caused by degenerative changes in the structure of one or more of the discs in between the cervical vertebrae. Common symptoms of discogenic pain include pain in the neck when turning or tilting the head. Pain may be worsened when the neck is held in one position for prolonged periods, such as when driving, reading, or working at a computer. There is often associated muscle tightness and spasms. Discogenic pain can also cause referred pain or odd sensations into the arm or shoulder.
Cervical facet osteoarthritis — The facet joints are located on sides of the vertebrae, and arthritis in this area can cause pain in the middle or side of the neck; some people also notice pain in the shoulders, around the shoulder blades, at the base of the head, into the ear and jaw,
or in one arm. A common cause of pain due to cervical facet arthritis includes a job or other activity that requires repeated extension of the neck (tilting of the head backwards).
Whiplash injury — “Whiplash” is a term used to describe injury caused by a traumatic event that causes an abrupt forward/backward movement of the neck. The most common cause of whiplash is a motor vehicle accident. similar injuries can occur in sports, when there is a significant blow to the body and the neck has to control the motion of the head. Whiplash can affect many structures in the neck, including the muscles, ligaments, and joints. Symptoms of whiplash can include severe pain, spasm, headaches, ear pain, jaw pain, and loss of range of motion in the neck.
Cervical myofascial pain — Myofascial pain is a disorder that causes tight and tender areas of muscle that are sensitive to pressure. Myofascial pain in the neck can develop after trauma or can occur with other conditions, such as psychologic stress, anxiety, depression, or insomnia.
Diffuse skeletal hyperostosis — Diffuse skeletal hyperostosis (DISH) is a syndrome in which there are abnormal calcifications (bone deposition) in the ligaments and tendons along the cervical spine, causing these tissues to become hardened. Most people with DISH have no symptoms while others develop stiffness, loss of mobility, and pain. This condition can also involve the thoracic (middle) and lumbar (lower) spine.
Cervical spondylotic myelopathy — Cervical spondylotic myelopathy occurs when the degenerative changes cause narrowing of central spinal canal. This narrowing leads to injury of cervical spinal cord or cause it to function improperly. In addition to pain and loss of motion, signs of cervical spondylotic myelopathy may include a variety of neurologic complaints. Weakness, difficulty walking or coordinating movement, inability to empty or control the bowels or bladder, and sexual dysfunction (erectile dysfunction) may occur as a result of irritation of the spinal cord.
Cervical radiculopathy — Cervical radiculopathy occurs when a nerve root is irritated by something pressing on it (eg.a protruding disc, arthritis of the spine, or a mass or cyst). Symptoms of radiculopathy can include pain, weakness, or changes in sensation (such as numbness or tingling) in the arms .The most common causes of cervical radiculopathy
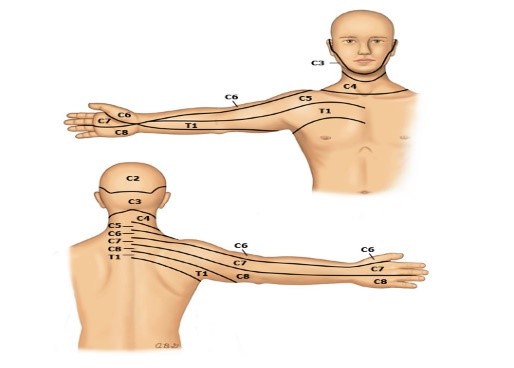
include:
- Degenerative changes related to aging or injury
- Herniation of a cervical disc
TESTS TO EVALUATE NECK PAIN
If you have persistent neck pain, you should see neurosurgeon for evaluation. They can try to determine the cause of your pain and recommend treatment. You should also see your neurosurgeon right away if you have severe pain, experienced a serious head or neck injury, loss of control to bowels or bladder, or have numbness or changes in sensation in your arms or legs.
Neurosurgeon will observe your ability to move your head to the left and right, forward and backward, and side to side. They will also observe your posture and the movement of the neck and shoulders, and feel the muscles in your neck, head, upper back, and shoulders to detect areas of pain or tension. They may conduct strength, sensation, and reflex testing as well.
Most people with neck pain will not need an imaging test. But in some cases, an imaging test (such as an X-ray, computed tomography [CT] scan, or magnetic resonance imaging [MRI]) or tests to check the muscles and nerves (such as electromyography [EMG]) will be recommended. Whether you need tests and which tests are recommended depends on your age, symptoms, medical history, and examination.
CONSERVATIVE TREATMENTS FOR NECK PAIN
In most cases, neck pain can be treated conservatively with over-the-counter pain medications, ice, heat, massage, and strengthening and/or stretching exercises at home. If you still have pain or restrictions in movement restrictions after a few weeks of conservative treatment, see your health care provider for further evaluation.
Pain relief — Acetaminophen or a nonsteroidal anti-inflammatory medication (NSAID) such as ibuprofen or naproxen may help relieve mild to moderate neck pain. Ice — For some people, ice applied to the sore area can help relieve neck pain. In general, for acute injuries, ice is recommended as the initial treatment for 3 days, especially if swelling is present.
You can also relieve muscle tightness by placing a bag of ice, bag of frozen vegetables, or a frozen towel to the painful area. The cold source should be wrapped in a thin dry cloth layer before it is placed on the neck to protect the skin. The ice or cold pack should be left in place for 15 to 20 minutes to deeply penetrate the tissues; this can be repeated every two to four hours until symptoms improve.
Skin damage can result from excessive use of ice, especially in people with poor skin sensation; it’s a good idea to inspect your skin each time you apply ice. Look for changes in pigmentation (for example, lighter- or darker-coloured areas) and let your health care provider know if you notice any problems.
Heat can also help to reduce neck pain in some people. Apply moist heat for 10 to 15 minutes with a shower, hot bath, or moist towel warmed in a microwave. If you use a heated towel, be careful not to overheat, as this can cause skin injury.
Stretching exercises — helps to restore and preserve your range of motion. Range of motion exercises and stretching may help decrease pain from muscle injury. It is best to perform stretching exercises when the muscles are warm, such as after the application of heat, or after a few minutes of cardiovascular warm-up exercises.
Exercises better be done in the morning to relieve stiffness and again at night before going to bed. Expect mild, achy muscle pain if you are new to exercise. If you have sharp or “electric” type pain in your shoulder or arm, tell your provider.
If you had a serious neck injury, do not try any new exercises or stretches before talking to doctor. Also, do not attempt these exercises if you have a pinched nerve in your neck, especially if there is pain or numbness into the arm and hand, unless recommended by a health care provider. While these exercises can dramatically improve symptoms of a pinched nerve, they can actually make the problem worse if done improperly.
Before doing stretching or strengthening exercises, it’s a good idea to warm your neck and upper back muscles by taking a warm bath or shower or applying a heating pad or moist, warm towel. Exercises are most effective if you do them twice a day, in the morning and before bed.
Exercises include:
- Neck rotation – Slowly look to the right. Hold for a few seconds. Look straight ahead and rest for a few seconds. Repeat 10 to 15 times, then perform on the left side.
- Neck tilting – Look straight forward, then tilt the top of your head to the right, trying to touch your right ear to your right shoulder (without raising your shoulder). Hold for a few seconds, then return your head to the centre. Repeat 10 to 15 times, then perform on the left side.
- Neck bending – Tilt your head forward and try to touch your chin to your neck using a nodding motion. Hold for a few seconds, breathe in gradually, and exhale slowly with each exercise. Exhaling with the movement helps relax the muscles. Repeat 10 to 15 times. Relax your neck and back muscles with each neck bend.
- Shoulder rolls – In a sitting or standing position, hold your arms at your sides with the elbows bent. Try to squeeze your shoulder blades together. Roll your shoulders backwards 10 to 15 times, moving in a rhythmic, rowing motion. Proper neck alignment posture is important during this exercise. Rest, then roll your shoulders forwards 10 to 15 times.
- Scapular retraction – While seated, hold your head in a neutral position and draw your shoulder blades backward (toward each other). Hold for 10 seconds, then relax. Repeat 10 to 15 times.
- Deep neck flexor strengthening – Lie on your back, on a flat surface, then draw your chin down (toward your chest) and inwards while contracting the deep muscles of your neck. For initial exercises, keep your head in contact with the ground and just “tuck.” Hold for five seconds, then relax. Repeat 10 to 15 times.
- Chest wall stretches – Stand in a doorway and hold your arms out to your sides with your elbows bent and your palms facing out. Place your elbows against the door frame, slightly below shoulder level. Then lean your chest forward while keeping your head in a neutral position as you slowly stretch your shoulder and chest muscles. Hold the stretch for 20 to 30 seconds, and repeat 10 to 15 times.
Stress reduction — Emotional stress increases neck tension and interferes with or delay the recovery process. Reducing stress may help to prevent neck pain from recurring. Relaxation techniques can relieve musculoskeletal tension. An example of a relaxation exercise is to take a deep breath in, hold it for a few seconds, and then exhale completely. Breathe normally for a few seconds, and then repeat.
Other activities that may help to reduce stress include meditation, mindfulness-based stress reduction programs, cognitive behavioural therapy, or progressive muscle relaxation.
Posture — can help prevent or reduce neck pain by doing activities and using positions that emphasize a neutral neck position and minimize tension across the supporting muscles and ligaments. Extremes of range of motion and positions that cause constant tension should be minimized or avoided.
It may help to:
- Avoid sitting in the same position for prolonged periods of time. If you work at a desk, try to take periodic five-minute breaks throughout the day. Avoid looking up or down at a computer monitor; adjust it to your eye level. Visual changes or new glasses prescriptions can also affect the way you hold your head and neck to read.
- Avoid putting pressure on your upper back with things like backpacks, over-the-shoulder purses, or carrying children. Alternatives may include wheeled backpacks or cases and having a child walk or ride in a stroller.
- Avoid doing overhead work for prolonged periods at a time.
- Maintain good posture by holding your head up and keeping your shoulders back and down. Try to keep your neck in line with your body and avoid hunching forward. Pay attention to your neck and arm position when you are using your phone.
- Use the car or chair arm rests to keep your arms supported. Find the optimal seated alignment in your car for your entire spine and make sure the head rest is at a comfortable position for your neck.
- Sleep with your neck in a neutral position by using a small pillow under the nape of your neck (if you sleep on your back) or sleeping with enough pillows to keep your neck straight in line with your body (if you sleep on your side). If you sleep on your back, putting a pillow under the knees can help to flatten the spine and relax the neck muscles. Avoid sleeping on your stomach with your head turned to one side.
- Carry heavy objects close to your body rather than with outstretched arms.
OTHER TREATMENTS
Many other treatments have been studied for neck pain. Some have limited evidence for benefit, while others are appropriate in certain situations (such as people with severe or chronic pain or certain types of neck injury). If conservative treatments are not effective, your health care provider might suggest trying one or more of the following.
Prescription pain medications — As discussed above, treatment with an over-the-counter pain reliever such as a nonsteroidal anti-inflammatory drug (NSAID) or acetaminophen may be enough to reduce your neck pain.
If your pain is not relieved with NSAIDs or acetaminophen, or if you have severe muscle spasm, your doctor might prescribe a muscle relaxant. If your pain continues to be severe, they may also consider prescribing tramadol, a stronger pain medication, for a short time..
If pain continues beyond six weeks despite treatment with tramadol (or in people who cannot or should not take tramadol), or if pain is disrupting sleep, certain antidepressant medications may be recommended.
Add-on treatments that may be helpful — While there is limited evidence for therapies like massage and acupuncture in the treatment of neck pain, some people find that they are helpful (at least in the short term), and they are unlikely to be harmful.
Movement-based therapy — Depending on your situation, your health care provider might recommend working with a therapist or athletic trainer to develop an individualized exercise program. This typically involves a combination of stretching, strengthening, and stabilizing exercises. A physical therapist can teach you exercises that you can continue to do at home between treatments.
Some people find activities with a mind-body focus, such as Tai Chi and yoga, to be beneficial. Whatever exercise program you follow, the goal is not only to improve pain but to help you regain function and be able to do your normal daily activities. In addition, staying active can help reduce stress and anxiety.
Spinal manipulation and other manual therapy — “Spinal manipulation” is a technique sometimes used by chiropractors, physical therapists, doctors, massage therapists, and others to relieve neck or back pain; it can be effective when used in conjunction with exercise. Manual therapy and joint mobilization are gentle types of manipulation that can help improve joint and soft tissue movement and flexibility.
While some people find that spinal manipulation helps with their pain, some studies have found that treatments that include quick “thrusting” of the neck are associated with a possible risk of serious injury. Aggressive manipulation or adjustments to the cervical spine should be avoided in people with certain conditions including cervical stenosis, cervical spondylotic myelopathy, or cervical radiculopathy.
If you are interested in trying spinal manipulation, talk with your doctor to make sure it is appropriate for you.
Trigger point injections — This involves injecting a local anaesthetic medication (such as lidocaine) into the muscles at specific areas of tenderness.
Trigger point injections may be recommended if conservative treatments do not significantly improve pain. However, there is no good evidence that trigger point injections help to reduce pain or speed healing in the long term. Trigger point injections with steroids into the neck muscles are not recommended due to the risk of injury to the muscles and lack of additional benefit.
Psychological and mind-body therapies — People with chronic neck pain may benefit from something called cognitive behavioural therapy (CBT). CBT involves learning about your condition (including addressing any misconceptions and fears that you may have about your pain), learning how to develop a more positive way of thinking, and setting activity goals and working toward those goals. CBT techniques may be performed by a psychologist or other trained professional.
Some people also find that something called “mindfulness-based stress reduction” helps. This involves attending a program virtually or in-person to practice relaxation and meditation techniques with someone trained in this approach. It helps in improving your ability to relax, cope with stress, and help manage your pain.
Treatments not routinely recommended — You may have heard of other treatments that claim to relieve neck pain. Unfortunately, most of these have not been proven to work or are only effective in specific situations. Examples include:
- Cervical collar – A soft cervical collar is a piece of foam covered with fabric that is worn around the neck to support the head. While occasional brief use of a collar may be helpful in certain situations (for example, if you have periods of increased pain that interfere with sleep), long-term or routine use is discouraged as this may delay recovery or allow the neck muscles to weaken.
- Cervical traction – Cervical traction involves the use of weights to realign or pull the spinal column into alignment. Clinical studies have shown no benefit from traction in the treatment of neck pain.
- Electrical stimulation – Transcutaneous electrical nerve stimulation (TENS) is a treatment that involves applying a mild electric current to the skin with the goal of decreasing pain and increasing mobility and strength. Evidence for its efficacy is mixed; your health care provider can talk to you about this approach if you are interested in trying it.
- Surgery – Surgery is not useful for treating most types of neck pain. However, surgery may have a role in relieving symptoms related to a pinched nerve caused by a herniated disc (cervical spondylotic myelopathy or cervical radiculopathy) if conservative therapy is not effective.
- If you have chronic neck pain that does not improve over time, your provider may refer you to a Neuro-spine specialty clinic.
If you want to try any new form of treatment, or have questions about approaches not discussed here, it is always best to talk with your neurosurgeon first. They can assess your situation and recommend treatments that have been proven to be effective.

DR. RAVIRAJ S GHORPADE MBBS,MCH(Neuro,NIMHANS)
CONSULTING BRAIN & SPINE SURGEON
BHS LAKE VIEW GROUP OF HOSPITALS
BELGAVI